Atherosclerotic vascular disease is a chronic condition that develops due to complex interactions of genetic, environmental, and lifestyle factors.
Epidemiological data indicate that cardiovascular diseases are the most common cause of increased mortality. Therefore, preventive actions based on current knowledge and epidemiological data on the prevalence of various risk factors in different populations with different baseline cardiovascular risks are essential. One of the tools for individual cardiovascular risk assessment is the SCORE-2 scale (Systematic COronary Risk Evaluation 2), which is used to predict the 10-year risk of death from cardiovascular diseases in Europe. SCORE-2 is an updated version of the original SCORE model and was developed by the European Society of Cardiology (ESC) to adapt to the changing epidemiological situation and newer data on cardiovascular risk.
To estimate the 10-year risk of all cardiovascular incidents for an individual using the SCORE-2 risk scale, one must first determine the appropriate country group according to the division proposed by the ESC (Poland belongs to countries with high population cardiovascular risk). Then, based on the individual’s clinical characteristics, using the appropriate risk table for that country, find the suitable cells for gender, smoking status, and (nearest) age. The table then contains cells with the closest value corresponding to systolic blood pressure and non-HDL cholesterol concentration. Risk estimates should be adjusted upward as a person approaches the next age category.
For example, in the 50–69 age group, a 10-year risk threshold of 5% for death from cardiovascular diseases estimated using the previous SCORE algorithm corresponds to an average 10-year risk threshold of death and development of non-fatal cardiovascular diseases at 10% estimated with SCORE2. This is because approximately the same number of people exceed the risk threshold and would qualify for treatment based on the newer scale. At the same time, considering only fatal cardiovascular events may underestimate the total burden of cardiovascular diseases, which in recent decades have affected non-fatal cases, especially in younger individuals. For instance, the 10-year risk of cardiovascular diseases for a 50-year-old male smoker with a systolic blood pressure of 140 mmHg, total cholesterol concentration of 5.5 mmol/l, and HDL-cholesterol of 1.3 mmol/l is 5.9% in low-risk countries, and 14.0% in very high-risk countries. Similarly, the 10-year risk for a 50-year-old woman with the same risk factor profile ranges from 4.2% in low-risk countries to 13.7% in a very high-risk countries.
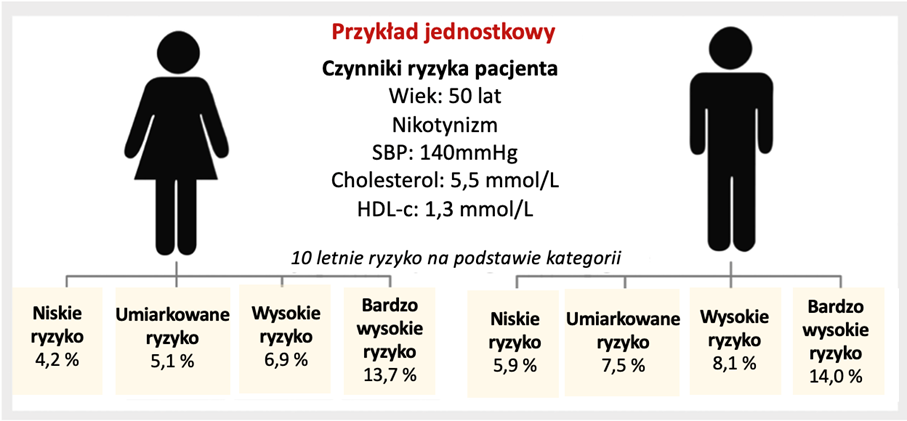
Figure 1. An example of risk assessment based on the SCORE2 scale for individuals living in regions with varying cardiovascular risk categories.
It’s important to note that the risk cut-off levels for these categories differ numerically for different age groups to avoid underestimating the need for treatment in younger individuals and overtreatment in older individuals. Age is a significant risk factor for cardiovascular diseases, and the benefits of controlling risk factors throughout life are more significant in younger individuals. Therefore, the risk thresholds for considering the start of pharmacological intervention are lower in younger people. At the same time, the risk categories do not directly translate into recommendations for immediate initiation of treatment.
Based on: SCORE2 working group and ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J 2021;42:2439/2454.